I had written on how a life of a doctor is changing gradually with increasingly demanding patients and patients who do not hesitate to take any action against you, over here and here . I had also written about doctor’s dilemma over here, here and here. I just had a chat with a medico-legal lawyer and what I heard from him is rather scary and I can see where the future is heading for medical doctors. The number of legal cases against doctors seem to be increasing by leaps and bounds. The number of complains against doctors to MMC is also increasing day by day. This could be the reason why the government is making it mandatory for doctors to have indemnity insurance in order to renew your APC from next year onwards. Whether this fee will be paid by the government for government doctors still remains to be seen.
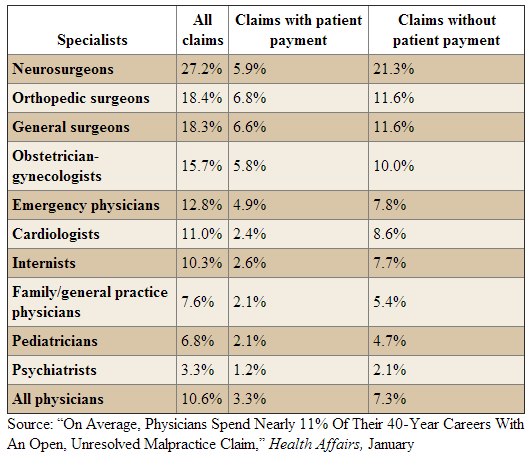
In US, doctors spend almost 10-30% of their entire career on medicolegal claims as mentioned in the table below. The highest was Neurosurgeons followed by Orthopaedic surgeons and General Surgeons. Even though more than half of it may not end up with a claim but the hassle that you have to go through will affect your life, your reputation and your daily practise. That’s the reason some doctors retire early in many developed countries. This is also the reason why doctors in US practices CBM ( Cover Backside Medicine) by doing all sorts of investigations to cover themselves. The situation will eventually be the same over here as you can already see it happening in major towns especially in Klang Valley. The very patient that you tried to help will turn against you. This is despite a flat salary growth for physicians in US over the years as mentioned here and attached below. It is the same over here where most doctor’s income are gradually dropping, especially in bigger towns.
The medico-legal lawyer that I spoke to represent one of the largest legal firm which handles medico-legal cases. The sentence ” patients are your worst enemies” was mentioned by him! When you least expected, a letter will reach your doorstep for a claim! That’s when your nightmare begins……………..
Physicians See Relatively Flat Salary Growth
Nov 28, 2012
“Possible explanations include managed care growth, Medicaid payment cuts, sluggish Medicare payment growth, or bargaining by insurance companies,” the authors write.
Dr. Seabury and colleagues also analyzed trends in wages, calculated as annual earnings (total annual labor income plus business income minus expenses) divided by number of hours worked. Adjustments were made for age, sex, race, and state of residence. In the years 2006-2010, median physician wage was $67.30 (interquartile range [IQR], $43.30 – $80.10) per hour, but dentists made $69.60 (IQR, $44.80 – $97.50) followed by pharmacists at $50.60 (IQR, $40.40 – $58.60), registered nurses at $29.90 (IQR, $22.8 0 – $38.50), and physician assistants at $31.20 (IQR, $20.80 – $43.80).
At the same time, healthcare and insurance executives earned a median $100,000 (IQR, $63,100 – $144,461) per year and $42.50 (IQR, $29.30 – $62.30) per hour in 2006-2010.
These findings emerge from an analysis of the Current Population Survey database from 1987 to 2010, with multiple years grouped together to smooth annual fluctuations in earnings and wages. When comparing median physician income from 1987-1990 ($143,963) to 2006-2010 ($157,751), a significant increase of $13,788 (9.6%) was seen (P < .001).
A total 30,556 healthcare professionals responded to the survey during this period, including 6258 physicians (20.5% of the total). To avoid potential earnings bias from trainees, only data for workers older than 35 years were analyzed in this study. Information on physician specialty was not available. The data represent median figures and do not account for top earners in a particular healthcare field (US Census caps earnings to protect identities), which is a potential limitation.
One coauthor was supported by the National Institute on Aging. The authors have disclosed no other relevant financial relationships.
JAMA. 2012;308:2083-2085. Abstract

Fully agree..even though i am just a HO in a government hospital that serve the so called “VIP’ from government settings, i can see the new trend that do not believe doctor,even the specialist. i have some difficulties to serve them. some of them, mainly younger generation, maybe just have their first degree and just M41/U41, not even Dato or Tan Sri, requested to have venepuncture to be performed by medical officer or specialist. They knows their rights even though they have little education in the tertiary centres. I felt funny when these people in so called ‘VIP’ government hospital requesting venepuncture to be performed by MO/specialist. The MO/specialist also served them. Funny but true. Personally i dont mind it is a private hospital/clinic. Fully agree, in future, patients are our greatest enemies..
Medical students sued their medical school over tuition fee increase, poor grade, racial issue, feeling unhappy with the school’s quality, low practical training ( As a result, the former students say they’re saddled with student-loan debts, but can’t find jobs in the medical field )
http://news.google.com/newspapers?nid=1346&dat=19751020&id=n6wwAAAAIBAJ&sjid=pPoDAAAAIBAJ&pg=7252,5302084
http://www.gwhatchet.com/2012/02/02/ex-student-sues-medical-school-after-dismissal-from-program/
http://www.insurancejournal.com/news/southeast/2012/07/26/257054.htm
You can’t realy sue any medical college for not getting a job as NO university guarantees you a job. It is always stated in their brochure(somewhere small at the bottom!)
That first news story is from almost 40 years ago.
The other 2 news articles are about Physician Assistants, not medical students. PAs work in some US states and are like MAs in Malaysia, except they have to have a degree.
Yes I think you young doctors will need to accept the reality that patients these days are very demanding (knowledgeable i would say) and it will increase as more & more patients are educated (and internet savy.) They know their rights and they expect good treatment for what they are paying for.
I, like many of my friends always surf the internet regularly when we have any medical issues…before i visit the GP or even the specialist. Believe me there is so much information in the internet…that my GP doctors are not able to explain to me well. Sometimes even my specialist cant or dont tell me much…I HAVE TO PROMPT THEM WITH MY QUESTIONS. Maybe he has too many patients so he wants to get rid of me quickly…lol.
Over the years I can give you many examples, where GPs have diagnosed insufficiently or incorrectly. Even Specialists have diagnosed incorrectly or they subject you to unnecessary trials & errors & tests.
But I have accepted the fact the GPs or Specialist are only humans, they based their treatment for you only based on their best knowledge & experience..so they can be wrong too…so I have to hep them to help me.
I can give you many examples for my years…but i wont bore you guys. So what you young doctors, HOs included can do ….is to make sure you work hard and learn to be a good doctor..
(Btw…i am not a doc…but i have been reading Dr Paga’s blog for two years now….my daughter is a HO now….even she tells me too…that many of the MO and HO are quite lazy….some even graduated from Ireland.) So if you dont want to be sued….please try to become a damn good doctor.)
The internet overcomes information assymetry. It works both ways. We find it easier to judge politicians. Patients find it easier to judge doctors. etc. etc.
In one of your posts you said that it is safer to do A level , STPM and maybe AUSMAT. Which pre-u cpurse is better, for I heard that overseas uni prefer A level or AUSMAT than STPM although they claim that they treat them evenly?
And do you think Pharmacy is a profession worth investing my time in? A pharmacist in Guardians told me that she earns 5k-6k per month, I do not mind the long working hours, but I just can’t stand being stuck in a small pharmacy shop and sit at the same place, see the same workers everyday from morning till evening…
I love a challenging, difficult, risky, interesting and non-routine job. In which career do you think is the most ideal?
Thank you so much!
Challenging, difficult, risky, interesting & non-routine….sorry – not in healthcare
Almost every job will become a routine after some time. The same goes to medicine.
If you are planning to go overseas then do A level or Ausmat.
British universities will not accept any Australian pre-U course for medicine, A-Levels or STPM only for them (though they much prefer the former) unless things have changed in the past few years.
Australian universities will accept AusMat and A-levels and probably STPM.
Uk med schools do accept Australian Year 12 results, but of course subject to the usual personal statement, UKCAT/BMAT tests and interview. Once they accept you they will give a conditional offer based on the ATAR rank. I know someone who was offered on condition of ATAR96.
Generally, but not necessarily true.
As I said, things have probably changed then. In the late 90’s, admission tests for medical schools hadn’t caught on yet and I remember 2 different UK medical schools telling me that they would not accept Aussie Matriculation because they had enough qualified candidates with A-levels applying.
The admission/aptitude tests gives them another thing to look at in order to compare students with different pre-u qualifications.
Dear Jacqueline,
I know quite a few chain store pharmacists working in the malls of klang valley, all complained of long working hours and only off on alternate saturday and even during 1st day chinese new year they have to work (they are chinese) and they do not like this sort of arrangement. Basically they said they are shop assistants selling medicine but with good product knowledge. They are complaining that when family members and friends are not working during weekends, they hava to work and cannot join them for social gatherings or outings. When they are resting at home, everyone is working. But it is not easy to get jobs, so they stay put at these chain pharmacies. And it seems that their pay is not that high too as what you have posted (5k-6k), some told me in smalll pharmacy shops or some chain pharmacies, they only offer you a starting salary around 2k. I do not know how true it is. They claimed that since they cannot get a place in medicine, so they just go for pharmacy. Hope you do more research before deciding on which course to study. All the best to you.
This is of course expected and not surprising. Some doctors bring the “government hospital” attitude into private practice. They expect that the educated and well-to-do patients will act like the regular poor, uneducated, and submissive patients they see in government hospitals. They adopt a paternalistic approach to medicine, sometimes not even making eye contact with patients, or properly explain to patients. When a patient ask more questions, some of these doctors gets annoyed and term these patients as “demanding”.
If a bus driver makes a careless mistakes costing lives of people on the road and finally gets penalized legally, should a doctor be forgiven? If you invite a wall painter into your house to paint your walls, and he carelessly breaks your plasma TV, are you not going to ask for compensation?
Patients are not the doctor’s worst enemy. It is a doctor’s careless attitude and poor communication skills which is his/her worst enemy.
As a society progresses, they become more aware of their rights.
Probably the reason why medical schools in the UK and Aus (perhaps also NZ and US) have made communication skills as part of the course.
most medical schools nowadays have communication skills incorporated into their syllabus. Frankly, it does not make any difference. Communication skills should be thought in schools. Medical schools are too late to change a person!
hi Jaz, it is not only medical schools in the UK and Aus have communication skills as part of the course, Malaysian medical schools do the same too, if not all, at least most of them (both public and private universities).
agreed but in medicine, sometimes we can’t predict what will happen. Even in best hands things can go wrong.
Dear Jayso, I am a gov doctor. May I asked what do u mean by bring ‘gov hospital attitude’ to private practice? what do u mean by ‘gov hosp attitude’ ? I find ur statement very unpleasant. I serve my patients with all my heart. When they ‘gone down’ I share the pain of their families. Many of my colleague are also serves the public as best as they could. Everyone have the option of choosing where they want to go for treatment. Yes, we doctor are selling our service, and i do agree that customers are always right. But sometime customers can be a pain. We do not force pts to come to see us, and pt always have a choice to chose who they want to see. Of course, pt may not able to choice who they want to see in public hospital. But they always have to choice to go to other hospital beside public hospitals.
Firstly, great to hear that you serve pts with all your heart.
What I mean by government hospital attitude is : a consultant bringing his god-like complex where he can “touch and go” on patients in the wards and in the clinics into private practice. Similar to a Klinik Kesihatan MO bringing his “touch and go” service to his newly opened private clinic. Whereby these people adopt a PATERNALISTIC approach to patient care, thinking that patients should not question your treatment/management, and should place 100% trust in your judgement.
Patients have the right to choose their doctors, and they have a right to ask questions – or even “be a pain” as you have mentioned. They have a right to their own body, and in the end, the autonomy of the patient trumps your beneficence.
“We do not force pts to come to see us, and pt always have a choice to chose who they want to see. Of course, pt may not able to choice who they want to see in public hospital. But they always have to choice to go to other hospital beside public hospitals.”
This is another government hospital mentality. The idea of “Kalau tak suka, pergi private-lah.” As if the poor have a choice on which hospital they get to go to. Many nurses love using this phrase – especially when clinics get busy. Instead of using this phrase, one should be creative and figure out how to make the system more efficient.
This mentality – “we do not force patients to come to see us” is not only in the government hospital. It is also all other government services, including the place where you make passport, make IC, driving license etc. Thinking that you are doing others a BIG favor, and people are begging for your service. The only reason patients still go to public hospitals is because they have no choice due to financial constraints.
Dear mr Jayso, great to see your reply. I must say ur reply does point out lots of weakness in the gov service. I believe u are someone who deal with lots of gov service, may be urself is also a doctor. Pardon me if I am wrong here, but the way you penned it down seem to be a rather generalized.
Ay Jayso, ever thought it may be simple mathematics? “Touch and Go” as you call it. Well, look, if you’ve got close to 40 patients to cover in a morning as a consultant, you have got to expect that. Consultants make executive decisions after being briefed by the teams. You see it as hands off, but in reality, they are calling the shots based on feedback from the team (Registrars, residents/MO’s, and interns).
It’s nothing about being paternalistic. Do you even know what that word means?
At the ward level, say you’re looking after 20 patients.
Say you spend 15 minutes with a patient – keep in mind, only 5 minutes is actually spent with the patient, the rest is spent looking through notes, investigation results and getting feedback from the team, and then WRITING EVERYTHING DOWN. Now multiply that by 20…and viola one whole morning is gone.
Afternoons? Well that’s when plans get put into place. Correspondence / liasing with other hospitals, arranging tests, managing the new admissions etc.
Often doctors simply dont have the time to do unnecessary things. Doing so means going back late… fine for a day, but not days on end *yes we burn out too.
At the end of the day, as long as the right decisions are made and the plans are carried out then you have done your job as a doctor and can sleep easy at night – im sorry if your doctor didnt spend an extra 10 minutes explaining everything to you because that would be insane (trust me it builds up).
That’s where the private system comes in… Doctors (at the consultant level) there are SOLELY responsible for their patients..and the ratio of doctors to patients is better… so yeah, they will pay more attention to their patients and talk to them more.
” At the end of the day, as long as the right decisions are made and the plans are carried out then you have done your job as a doctor and can sleep easy at night – im sorry if your doctor didnt spend an extra 10 minutes explaining everything to you because that would be insane (trust me it builds up).”
Hi. Mint, how can a right decision be possibly made when feedbacks are based from the (Registrars, residents/MO’s, and interns) who MAY have t he same mentality like you ? that is to ‘shortcut’ everything because too many pts, so by the time these ‘shortcuts’ reach the consultant, it may become ‘super shortcuts’ which only represent 10% to 20% of the exact problem of the pt’s. It sounds so ‘ chi-cai’ and scary-lah!!
Mint Berry – look carefully at my post above.
Of course because of the sheer volume of patients, one has to adapt accordingly. What I was talking about was that your adaptation to the government hospital environment moulds you into a new person – and you bring that practice to your private practice, where even when you have more time – you still adopt your touch and go practice from government hospital into private practice. This is clearly evident if you have the opportunity to bring your mother to visit 2 separate consultants in private practice, one who completed his training in a western country, and one who complete his training in Malaysia. Though you may say it is inappropriate to make a generalized statement, that is what I can gather from my observation and experience. If someone wants to do a research on this topic, feel free to do so.
And yes, I know what paternalistic mean, and if you read my post carefully, it would be clear that my use of the word is appropriate – provided you know what paternalistic means.
In many clinics, there is no such thing as spending develop a cooperative approach to patient care. This is understandable in the government setting due to the cohort of patients there who may willingly hand over the decision making process to their doctors and also due to the lack of time, but this is unacceptable in private practice.
And as for your justification of “touch and go” based on number of patients in the government hospital, this is understandable.
Understandable, but not acceptable. The problem is in the system, and the people in the system. You may justify touch and go because limitation of time now , but when a you are sued in court because you directly or indirectly caused a baby prolonged hypoxia resulting in this child growing up with cerebral palsy, do you think the court is going to sympathize with your “simple mathematics of time”? I doubt so. Unfortunate for you, the problem is in the system, and you have to bear the consequences.
Hi curious,
You wrote: “how can a right decision be possibly made when feedbacks are based from the (Registrars, residents/MO’s, and interns) who MAY have t he same mentality like you ? that is to ‘shortcut’ everything because too many pts, so by the time these ‘shortcuts’ reach the consultant, it may become ‘super shortcuts’ which only represent 10% to 20% of the exact problem of the pt’s. It sounds so ‘ chi-cai’ and scary-lah!!”
Mint may answer this him/herself later, but I’m not sure if you completely understand how things work in public hospitals. There is a hierarchy. In general, junior staff (interns or house officers) will see the new patients as they get referred, order some investigations or initiate treatment, run the cases by their MO or registrar (or maybe do this first if they are inexperienced), and the consultant will see everyone on their round to make sure the right things are being done and make changes if necessary.
There are of course exceptions. In some cases, the consultant may be called to attend to the patient earlier. It is the consultant’s responsibility to ensure that their junior staff know what they are doing – and this may be done thru teaching on the round, weekly tutorial sessions,etc. The more faith a consultant has in their MO/registrar, the more they will allow independent practice.
The consultant cannot be expected to see every patient when they come in all the time. That would be like a factory manager working at the assembly line all the time. Just not feasible. This is how it is in public hospitals that have a British-based structure.
Now, the issue of incompetent or poorly-trained junior doctors is another thing altogether. A consultant can only educate the junior doctors in their team/department to a certain extent. The basics already need to be there and a good medical school should be able to teach these junior doctors to manage the ‘big things’ safely. If these basic knowledge and skills are missing or not taught well, then the whole system is at risk.
“This is clearly evident if you have the opportunity to bring your mother to visit 2 separate consultants in private practice, one who completed his training in a western country, and one who complete his training in Malaysia”
Hi Jayso, Speaking through my personal experiences with many consultants, I do not see any difference in one who completed his training in Malaysia with one who completed his trainings in western country (I am comparing those who are very senior ones in the reputable private hospitals in klang valley). They all willing to spend more time with me if they do not have many patients waiting outside their room. I always try to go slightly late and be the last few patients, they are obliged to answer any questions (even not related to their speciality).
Jayso, re-read what I posted. I was explaining things at the consultant level as patients think their treating doctor (consultant) doesnt spend enough time with them. There is no shortcut to doing a reasonably thorough examination of a patient and conducting appropriate workup. I was responding to this: “When a patient ask more questions, some of these doctors gets annoyed and term these patients as “demanding”.”
There is nothing “touch and go” with medicine, but if a consultant needs to see 40 patients in a morning that is what will happen. THE REST OF THE TEAM should ensure the appropriate workup actually happens – That’s what the registrars, MO’s and housemen are for.
Dont get me wrong:
Every patient deserves appropriate examination and workup. I was explaining the reason as to why consultants dont sit down and chat or do full physical examinations…. and why they get annoyed if patients demand they sit down and talk – this is more common than you think. It’s not because of some God complex or egomania – it’s simple time management.
Touch and Go medicine should never happen at the ground level. That’s where the competence of the crew is tested (MO’s, interns, registrars). Things are never touch and go and every patient should be fully examined and worked up.
Here’s what usually happens in Australia:
1) Registrars admit, and do a reasonably thorough focused examination. Documents plan. Liases with consultant if unsure.
2) Consultants breeze through ward rounds, not always examining the patient personally… especially on weekend covers. The point of my post is that this is NOT touch and go medicine
3) Interns/MO’s put plans into practice… making all the referrals, blood slips, tons of paperwork. Examines patients appropriately when called (again, not touch and go medicine)
Every patient gets an examination AND a plan. However some patients/families are just difficult and despite all plans put into place and appropriate examinations, will still constantly seek affirmation and attention…then rumble about how the consultants only spend minutes with them in the morning. They dont realize how much work goes on behind the scenes… or the time put in by the registrars and the rest of the crew.
I think a lot of medicolegal cases are due to poor communication between the doctors, hospitals and the patient. There is a difference of medical negligence and complication arise due to medical interventions. Many patient who have medical complcaiton thinks that medical complication is due to negligence but this is not true as every medical intervention carry some amount of risk. Communication prior to medical intervention will minimise these medicolegal problem.
yes, that’s why we should improve our consent forms
Consent forms can mean very little in court and are easily challenged. What’s more important is simple documentation of why things are done. And never, never, NEVER write down differentials in patient notes – you are recording that you thought about something in a legal document!
I hope they can be more thankful for the doctors rather than suing them.
Well, the sad reality is when doctors are a dime a dozen, patients can now be picky. Human nature, really.
that generation is gone or going…………
Hi Jacqueline….couldnt help commenting…..I have 2 children who went into medicine and dentistry…..and both regreting. now.. I did advise them to go into Pharmacy b4…but they thought it was inferior medicine & dentistry.
Pharmacy degree opens the doors to many professions….not just a Pharmacist in a pharmacy….eg manufacuring etc. In many manufacturings..it is a must to have a qualified pharmacist …government regulations.
You dont need to end up working shifts and odd hours as with medicine…when your friends are enjoying their weekends & public holidays ..you will be working.
Btw if u open an independent Pharmacy….its like a retail outlet….or minimarket…apartment from the controlled medicine …you can sell anything & everything….and be your own boss….depending on how hard you willing to work..u can expand and have a few outlets ..and make good money.
And best of all time is your own…you decide when you want to go to work…you can just emply staff to run your outlets…you just need to be around to dispense prescription medicines. Good luck to you.
Thank you for your posts!
…and again yesterday another Malaysian doctor convicted of sexual assault charges..somewhere in Australia… ( http://thestar.com.my/news/story.asp?file=/2013/2/18/nation/20130218164620&sec=nation)..
….What I heard, its more because of improper documentation….
Its the same person as before. Only now they come up with the decision etc.
Dear Dr Pagalavan,
How about : for future ( private ) doctors : step by step how to claim patient’s payment from medical insurance company
this is not done by doctors. It is done by the hospitals. Doctor’s charges are regulated by the government and the insurance companies follows it.
Agree with Dr. Pagalavan, patients today are much different from those as recent as 10 years ago, some are really well informed of their rights, but most don’t actually know too well, and tend to overstep their boundaries, thinking this is their right, that is their right, etc, when in fact they are not really that knowledgeable regarding their real rights. I am a general dental practitioner with a law degree and a further qualification in medical law, I have already had quite a few friends and seniors who had unpleasant ‘entanglements’ with patients.
Nowadays it is mainly a balance of medical paternalism vs patient autonomy, one of the best protection that any doctor can provide for himself is a relatively detailed knowledge of the law, as some patients tend to ‘bully’ the doctor who is unsure of certain aspects of law pertaining to the practice of medicine.
Ur very right . Getting bully by patients in gov sector is a norm for me. And nobody to back you up just because it will bring bad name to their department.But knowing your rights and knowing ur work really well saves u a lot of headache.
Hopefully the lawyer that you spoke to is not one of my bosses..:)
I do agree that with a click on the internet, the patients will get vast information on their conditions. The pros – patients are well informed; the cons – some of those information are not really accurate.
I had a doctor that informed me that his patient even start suggesting to him what he need to do to treat him..wonder why he still went and consult him giving the fact that he even taught the doctor on what to do.
And I do agree, the litigation cases against doctors are increasing.
i have had same type of patients as well. The moment they enter the room, they will request what they want based on their own “research”
[…] of doctors simply because many of their own citizens are not interested in being one. The high litigation rate and demanding population are some of the reasons quoted. Oh, don’t forget the high indemnity […]